
Having worked in 5 different cities across the world, it always amazes me the things people tell me that they were told about their health care. Sometimes it is a complaint about the medical information they were given and sometimes it is a complaint about bedside manner. I use the information to learn, grow and to become a better doctor. I usually don’t comment on what I am told as I was not present to hear the information first hand. And as everyone knows, things can be lost in translation. However, sometimes I hear and see things (firsthand) more than once and want to ensure that everyone out there is receiving the best information and care possible.
When we train as doctors, we are in an aggressive learning environment. Our knowledge is fresh and up to date. As we get out into practice, it takes conscious effort to stay this fresh. And with the recent advances in medicine, staying fresh can be tough. We all develop protocols and styles. These protocols we implement can become out of date quickly. Sometimes the out of date protocols do no harm which is what every good doctor strives for. But sometimes they can harm. The information I will present is up to date practice based on evidence. The myths are pooled from all of the locations I have worked in.
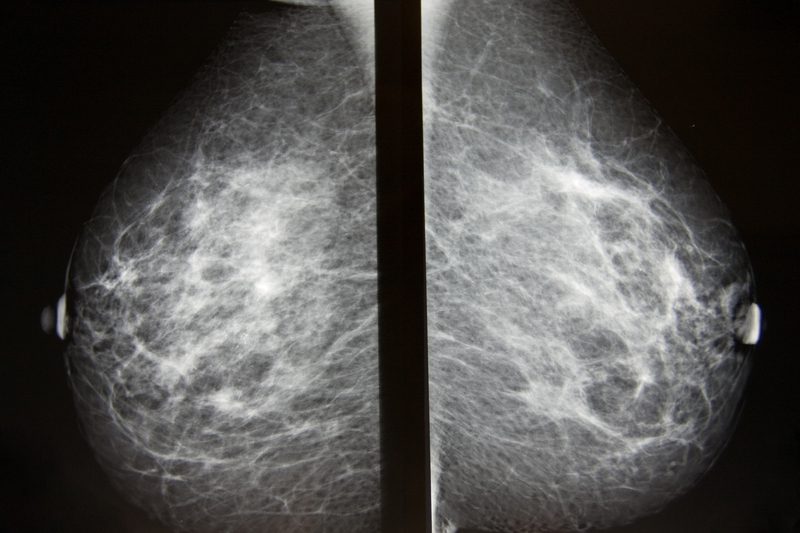
Medical Myth #1: A breast ultrasound is a good screening test alone for breast cancer.
Mammography is still considered the gold standard when screening (normal risk women) for breast cancer. Breast ultrasound alone is not a good screening test. It I used in conjunction with mammography when trying to characterize a breast lesion. Ultrasound can distinguish between a cystic and sold lesion and is used to provide guidance when performing biopsies. It is used first line in imaging in the following instances: pregnant women or women less than 30 years old who have a breast symptoms or findings on exam. The importance of screening is because breast cancer is the most common non-skin breast cancer. If you want more information about when to screen read my prior post here. Mammograms can be done plain film or digitally. Multiple studies have been done and there is no difference in detecting breast cancer for most women. Digital mammography was more accurate for premenopausal, perimenopausal women and women with dense breasts. While mammography is the best screening test for normal risk women, MRI screening in combination with mammography is emerging for high risk patients. Newer tests, such as tomography, are being studied as well.
Why important to point out: A women can be given a false information that she has been screened negative for cancer if she only has a breast ultrasound.

Medical Myth #2: Skull X-rays are indicated when evaluating severe (non traumatic) headaches.
If there is a need to further evaluate a patient who comes in complaining of a headache, then a head cat scan (with and without contrast) is usually the diagnostic test of choice. A skull x-ray offers no information about lesions within the brain. Some of the reasons for wanting to do further imaging are when a doctor detects an abnormal finding on neurologic exam, your headaches are rapidly increasing, you have developed a lack of coordination, you complain of the worst headache of your life, the headache wakes you from sleep or you have a history of localized neurologic complaints such as tingling or numbness.
Why important to point out: Ordering skull films delays the time to obtaining a cat scan if it is truly needed and in certain diagnosis time is of the essence.

Medical Myth #3: Elbow pain in a healthy early 30’s woman is due to osteoporosis.
In this instance, one might say maybe the patient misunderstood the doctor but the patient was clear. Even if the intent was to say the diagnosis was osteoarthritis, the patient’s age make this unlikely. Furthermore, the elbow is a non-weight bearing joint thus making degenerative processes like osteoarthritis exceptionally rare. Common things are common. In a healthy active woman, without a history of trauma, the pain is likely secondary to overuse. Among common diagnosis are: tennis elbow (hence the above photo), olecranon bursitis, nerve entrapment at the elbow and pain which is referred from a pinched nerve in the neck (radiculopathy).
Why important to point out? Treatment methods differ for different diagnosis and the patient may receive unnecessary medications.
Medical Myth #4: Sinus x-rays are indicated if a bacterial sinus infection is suspected or is not resolving with treatment.
Sinus x-rays are not indicated to diagnose a sinus infection. The decision to treat should be based on symptoms (see myth #5). If imaging is needed as may be the case with recurrent or chronic infections, the diagnostic test of choice is usually a noncontrast cat scan. Plain x-rays have both a high false negative and false positive rate.
Why important to point out? Sinus x-rays are unnecessary exposure to x-ray.
Medical Myth # 5: Antibiotics are needed in patients with acute rhinosinusitis.
The symptoms of acute rhinosinusitis aka acute sinusitis are: nasal congestion, purulent nasal discharge, maxillary tooth discomfort, and facial pain or pressure that is worse when bending forward, fever, fatigue, cough, ear pressure or fullness, headache, and halitosis.. The majority of patients with acute sinusitis are infected with a virus not bacteria. Acute bacterial infection occurs in only 0.5 to 2 percent of episodes of acute sinusitis. Bacterial infections require treatment with antibiotics. The Centers for Disease Control put together the following symptoms which are suggestive of acute bacterial rhinosinusitis: symptoms lasting 7 or more days with any of the following: purulent nasal discharge, tooth or facial pain located in the upper teeth, one sided sinus tenderness over the maxillary sinuses which are located below the eyes and adjacent to your nose or worsening of symptoms after initial improvement.
Why important to point out? Treating with antibiotics when not indicated can lead to resistance thereby rendering the antibiotics ineffective over time.
Medical Myth # 6: Progesterone (aka duphaston) is an effective therapy for PMS.
Progesterone and progestins which were once the most common therapy for PMS have been found to be ineffective in studies. Other remedies that have been found to be ineffective are evening primrose oil, essential free fatty acids and ginkgo biloba extract. Treatments which may be of benefit thought are: exercise and Vitamin B-6, oral contraceptives, Vitamin E, Calcium, magnesium, relaxation techniques and reflexology. If the above treatments fail, a class of antidepressants called Serotonin Reuptake Inhibitors (SRIs) is very effective.
Why important to point out? It can result in treatment with unnecessary medication.
Love to hear your global health care stories! Have you ever been told something that you didn’t think was quite right?












2 Comments to Global Medical Myths